
The current once-in-a-century COVID-19 pandemic highlights how deeply inequitable our world is. Being rich and famous comes with immense perks: leniency in the criminal justice system, access to educational opportunities, and access to quality healthcare.
In this age of information overload, we have greater insight into the lives of celebrities than those of our own neighbors — after all, we are their one million social media followers. We’re currently seeing an unacceptable disparity in access to COVID-19 testing between those whose lives are considered newsworthy and those whose lives are not. The roll call is long: actors Idris Elba and Tom Hanks, heads of state, and entire sports teams have managed to quickly get tested and receive results. Where is this robust and efficient testing apparatus for the rest of us?
In the UK, where I’m currently working as a doctor, debate around how to tackle the novel coronavirus has raged on, with little agreement beyond the merits of hand-washing and basic infection prevention and control (IPC). After weeks of articles and petitions, the prioritization of providing COVID-19 testing for healthcare workers and ensuring that they are well equipped and protected appears to be gaining traction. The UK government has mentioned stepping up testing, particularly of healthcare staff in several press conferences, but this has yet to be put in place nationally. Shortages of Personal Protective Equipment (PPE), logistical difficulties in delivering trainings on appropriate use, and rapidly changing protocol and processes have been discussed ad nauseum in healthcare circles.
Britain’s National Healthcare Service is underfunded, staff attrition is at an all-time high, and burn-out is commonplace. This isn’t news — it has been on the Brexit back-burner for two years and has now been ironically overshadowed by COVID-19. The general sense is one of unpreparedness despite the fact that positive cases were detected outside of China before the end of January and the first positive diagnosis in the UK came on January 31st. As I write this, the never-ending queue of staff in need of testing continues to build in the hospital where I work. Our occupational health office is tasked with both addressing staff concerns and providing COVID-19 testing services, all while continuing to play a critical role in staff on-boarding. Several staff, including myself, have been exposed and asked to self-isolate after developing symptoms. The likelihood that I will ever be tested is slim. My symptoms peaked before staff testing made it on the agenda and by day seven it will be a moot point.
Under-resourced healthcare systems
Many have questioned how low- to middle-income countries (LMICs) with already poorly resourced healthcare systems will cope. The short answer is they won’t.
The Ebola outbreak of 2014–2016 laid bare the gaps in fragile healthcare systems in West Africa. While the crisis left behind invaluable lessons and inter-process communication structures, the healthcare systems of many African countries are far from prepared for this pandemic. This is both a health problem and a socio-economic problem. The persistently high rates of infectious disease point towards entrenched infection control gaps — it’s hard to wash your hands regularly when necessities like soap and clean running water are not readily available or accessible. In settings where en-suite toilets are not a given, cramped accommodation is the norm, and routine health practices leave much to be desired, viral visitors can easily figure out how to get around.
The novel coronavirus is mainly spread by droplets, but it has also been noted to have faeco-oral transmission. In much of Sub-Saharan Africa, respiratory and gastrointestinal tract infections along with malaria are among the most common presentations to health facilities. This fact, combined with low doctor/nurse to patient ratios, general shortages of drugs and equipment, and Intensive Care Unit (ICU) beds in the single digits, paint a grim picture.
Proposed control strategies such as social distancing and restrictive lockdowns will disproportionately affect the socio-economically disadvantaged who need to be in public to make a living and feed their families. Affected countries such as Taiwan and Singapore instituted strict controls and have received praise for their quick action. However, the effects of a slow down in commercial activity are sources of both private and public concern in many countries. In the UK, the economy is heavily reliant on services, tourism, and a strong brand of being a stable country with a top-ranking currency. This makes a delay in enforcing what some have called ‘common sense’ distancing measures somewhat understandable. LMICs face a somewhat similar predicament with different dimensions. Their reliance on foreign imports and aid might vary from country-to-country, but compared to countries in Europe and some in Asia, most African nations have a low gross national income per capita.
Speaking of poverty…
One viral Tweet summed it all up: “How do you self-quarantine in an informal-settlement? Or in a household full of people? How do you ‘stock-up’, when you live from hand to mouth? What will business closures mean for daily/hourly waged workers? Asking for a continent.”
All over the globe, there’s been an outcry from contract/freelance/zero-hours workers who will suffer the most as stringent measures to fight the outbreak are put in place. Salaried workers are free to assume that they will get paid at the end of the month whether or not they remain in isolation but people who subsist on daily wages do not have that luxury. Sadly, a significant percentage of the African workforce is in the informal sector. Combine this with a generally low uptake of financial services and poorly developed welfare systems and things begin to look quite bleak. It’s been interesting to see several African countries such as Rwanda, Uganda, and South Africa acting swiftly to adopt tight travel restrictions and social distancing practices better, in some cases, than their compatriots in the Global North. Yet some countries like my native Ghana appear to hedge their bets: banning all social gatherings and ironically allowing establishments such as bars and night clubs to still operate. Closing schools but allowing exams to proceed, and requiring offices and business, in general, to go about activities normally with the caveat that ‘social distancing’ protocols are observed.
The Silver Lining
In possibly equal parts ignorance and denial, I’ve heard firsthand from relatives that this pandemic is nothing to worry about because “if it’s your time to die, it’s your time to die” and “the virus doesn’t like heat.” I can say that with every newly confirmed case, the African mantra of immunity is waning. For every piece of advice on prevention and mitigation there are hundreds of dissenting voices who say it won’t work in [insert country here] and thousands of sourceless forwarded WhatsApp messages. To them I say: We need to own our limitations. We will not survive this pandemic because of our short comings but in spite of them. We live in volatile and uncertain times and this is nothing new.
People living in LMICs grapple with shortages, unreliable supply chains, and unpredictable amenities such as electricity on a daily basis. Panic mode stockpiling three years worth of toilet paper for potentially a two-week quarantine might be something new where I now live in the UK, but storing water in re-fashioned 70 gallon drums and reusing run-off bath water to flush toilets was commonplace for me growing up.

We Africans are more than prepared to deal with the uncertainty that COVID-19 will bring. Coups d’etat and civil unrest are unfortunately the rule and not the exception in Africa’s political history so curfews and limitations on free movement are again, nothing new. Postponed exams and disrupted educational calendars due to leaked exam questions and strikes? Again, an occurrence — while annoying and disruptive — that is not uncommon. What’s a three-month delay in a pandemic? I’m not condoning what may or may not be an example of what not to do during the pandemic, but a viral dance craze about a virus? Joie de vivre — live joyfully.
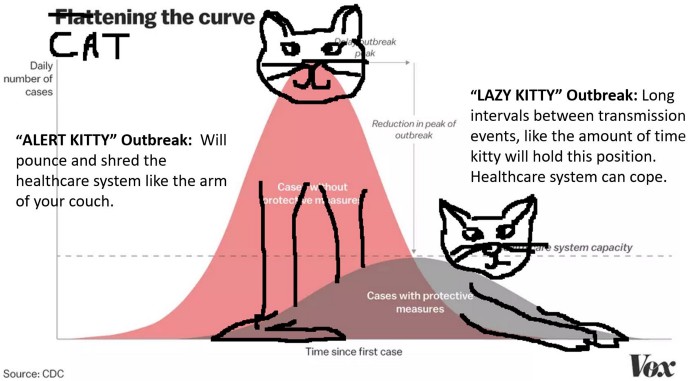
If the data tells us anything, getting a handle on the first few cases is critical. Strict enforcement of a 14-day lockdown when you have a handful of cases might make the difference between halting spread in its tracks and playing catch up for the next six months. One of the benefits of “flattening the curve” is keeping the number of people affected at a manageable state. Countries with under-resourced health systems should be the first ones striking the lazy kitty pose.
This article was first published on Amplify.
Sandra Danso-Bamfo was a 2015–2016 Global Health Corps fellow. She is currently a Trust Doctor at Darent Valley Hospital in the UK.
Global Health Corps (GHC) is a leadership development organization building the next generation of health equity leaders around the world. All GHC fellows, partners, and supporters are united in a common belief: health is a human right. There is a role for everyone in the movement for health equity. To learn more, visit our website and connect with us on Twitter/Instagram/Facebook.
